Submission: 01 January 2026 | Acceptance: 20 February 2026 | Publication: 24 April 2026
Dr Tahmoor Ghori1, Dr. Ameet Kumar Lalwani2, Dr Asad Jahangir3, Dr Ahmad Haroon4, Dr Qasim Raza5, Dr Faiza Maqsood6
1Lecturer, Fazaia Ruth Pfau Medical College, Karachi
2Associate Professor, Sindh Institute of Urology and Transplantation, Karachi Pakistan
3Senior Lecturer, Directorate of Education Development, Ziauddin University
4Assistant Professor, Bahria University Health Sciences Campus, Karachi
5Professor of Medicine, and Dean Shahida Islam Medical College, Lodhran
6Assistant Professor, Shahida Islam Medical College, Lodhran
ABSTRACT:
Background: Pulmonary nodules were commonly detected on imaging, posing a diagnostic challenge in distinguishing benign from malignant lesions. Accurate and early differentiation was essential for appropriate clinical management and prognosis. Dual-energy computed tomography (DECT) had emerged as an advanced imaging modality, providing functional and material-specific information that could improve diagnostic accuracy compared to conventional CT.
Aim: This study aimed to evaluate the diagnostic value of dual-energy CT in differentiating benign and malignant pulmonary nodules.
Methods: This cross-sectional study was conducted at Shifa International Hospital, Islamabad, from March 2025 to February 2026. A total of 110 patients with radiologically detected pulmonary nodules were included. Patients underwent dual-energy CT scanning using a standardized protocol. Quantitative parameters, including iodine concentration, effective atomic number, and spectral attenuation curves, were analyzed. Final diagnosis was confirmed through histopathology or clinical follow-up. Sensitivity, specificity, and diagnostic accuracy of DECT parameters were calculated to assess their effectiveness in differentiating benign from malignant nodules.
Results: Out of 110 pulmonary nodules, 62 (56.4%) were malignant and 48 (43.6%) were benign. Malignant nodules demonstrated significantly higher iodine concentration and steeper spectral attenuation slopes compared to benign nodules (p < 0.001). The sensitivity and specificity of DECT in differentiating malignant nodules were 90.3% and 85.4%, respectively, with an overall diagnostic accuracy of 88.2%. The combination of multiple DECT parameters further improved diagnostic performance. DECT showed a strong correlation with histopathological findings, reducing the need for invasive diagnostic procedures.
Conclusion: Dual-energy CT was found to be a highly reliable and non-invasive imaging modality for differentiating benign and malignant pulmonary nodules. Its ability to provide quantitative and functional information significantly enhanced diagnostic confidence and could aid in early and accurate clinical decision-making.
Keywords: Dual-energy CT, Pulmonary nodules, Benign lesions, Malignant lesions, Diagnostic accuracy, Iodine concentration, Spectral imaging.
INTRODUCTION:
Pulmonary nodules were commonly encountered abnormalities in thoracic imaging and represented a significant diagnostic challenge in clinical practice. With the widespread use of advanced imaging techniques, particularly computed tomography (CT), the detection rate of pulmonary nodules had increased substantially over recent years. These nodules could be broadly classified into benign and malignant categories, with the latter often representing early manifestations of primary lung cancer or metastatic disease [1]. Early and accurate differentiation between benign and malignant pulmonary nodules was therefore considered crucial, as it directly influenced patient management, prognosis, and survival outcomes.
Traditionally, the characterization of pulmonary nodules relied on morphological features observed on conventional CT imaging. Features such as size, shape, margin characteristics, and internal composition were used to estimate the likelihood of malignancy. Benign nodules were often associated with smooth, well-defined borders and smaller sizes, whereas malignant nodules tended to exhibit irregular or spiculated margins and larger dimensions [2]. However, there had been considerable overlap in these imaging features, which limited the diagnostic accuracy of conventional CT. In many cases, benign lesions such as granulomas or hamartomas could mimic malignant nodules, while early-stage malignancies could present with relatively benign appearances [3].
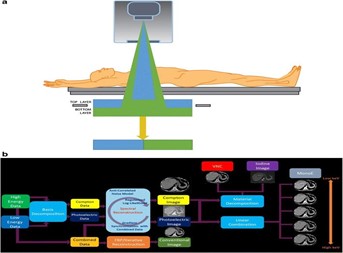
The introduction of dual-energy computed tomography (DECT) had represented a significant advancement in imaging technology, offering new possibilities for improved tissue characterization. Unlike conventional CT, which utilized a single X-ray energy spectrum, DECT employed two different energy levels to acquire imaging data. This approach enabled the generation of multiple image datasets, including virtual monochromatic images and material decomposition images, such as iodine and water maps [4]. The underlying principle of DECT was based on the fact that different tissues exhibited distinct attenuation properties when exposed to varying energy levels, allowing for more precise differentiation of tissue composition.
One of the key advantages of DECT in the evaluation of pulmonary nodules was its ability to provide quantitative parameters that reflected the biological and vascular characteristics of lesions. Parameters such as iodine concentration, effective atomic number, and spectral attenuation curves had been shown to differ significantly between benign and malignant nodules [5]. Malignant lesions typically demonstrated increased vascularity and higher iodine uptake due to neo angiogenesis, whereas benign lesions often showed lower or more heterogeneous enhancement patterns. These quantitative measurements provided additional diagnostic information beyond conventional morphological assessment and contributed to improved differentiation accuracy.
Furthermore, DECT had facilitated the reduction of imaging artifacts and improved image quality through monochromatic imaging [6]. Studies had demonstrated that images reconstructed at optimal energy levels, such as 70 keV, offered better contrast resolution and reduced noise compared to standard CT images. This enhancement in image quality allowed for more reliable evaluation of subtle lesion characteristics and improved the extraction of radiomic features. Radiomics, which involved the high-throughput extraction of quantitative imaging features, had further expanded the diagnostic potential of DECT by enabling the assessment of tumor heterogeneity and microstructural patterns that were not visible to the human eye [7].
In addition to structural and compositional analysis, DECT had also shown promise in evaluating perfusion-related parameters of pulmonary nodules. Perfusion CT techniques, including dual-input analysis, had demonstrated significant differences in blood flow characteristics between benign and malignant lesions. Malignant nodules typically exhibited increased perfusion indices due to abnormal vascular proliferation, whereas benign lesions showed relatively lower perfusion values. These functional insights further complemented anatomical and compositional data, enhancing the overall diagnostic capability of DECT.
Despite these advancements, the differentiation of benign and malignant pulmonary nodules remained complex, and no single imaging modality could provide absolute diagnostic certainty. However, DECT had emerged as a promising non-invasive tool that combined morphological, functional, and quantitative imaging parameters into a single comprehensive assessment. Its ability to improve diagnostic confidence, reduce unnecessary invasive procedures, and guide clinical decision-making had made it an area of growing interest in thoracic imaging research.
Therefore, the present study was conducted to evaluate the diagnostic value of dual-energy CT in differentiating benign and malignant pulmonary nodules, with a focus on its quantitative imaging parameters and potential to enhance diagnostic accuracy in clinical practice.
MATERIALS AND METHODS:
This prospective observational study had been conducted at Shifa International Hospital over a period of one year, from March 2025 to February 2026. The study aimed to evaluate the diagnostic value of Dual-Energy Computed Tomography (DECT) in differentiating benign and malignant pulmonary nodules. A total of 110 patients presenting with pulmonary nodules detected on initial imaging were enrolled in the study using a non-probability consecutive sampling technique.
Study Population
Patients aged between 18 and 80 years, who had been identified with solitary or multiple pulmonary nodules (measuring 5 mm to 30 mm in diameter) on chest radiography or conventional CT scan, were included in the study. Patients with prior history of lung malignancy, those who had undergone chemotherapy or radiotherapy, pregnant women, and individuals with severe renal impairment (contraindicating contrast administration) were excluded. Written informed consent had been obtained from all participants prior to enrollment.
Imaging Protocol
All enrolled patients underwent Dual-Energy CT scanning using a state-of-the-art dual-source CT scanner. The imaging protocol had been standardized for all patients. Scans were performed in the supine position during a single breath-hold to minimize motion artifacts. Both non-contrast and contrast-enhanced scans were obtained.
For contrast-enhanced imaging, an iodinated contrast agent was administered intravenously at a dose of 1.5 mL/kg body weight, followed by a saline flush. Dual-energy acquisition was performed using two different energy spectra (typically 80 kVp and 140 kVp). This allowed for material decomposition and generation of iodine maps, virtual non-contrast images, and effective atomic number (Z-eff) maps.
Image Analysis
The DECT images had been analyzed independently by two experienced radiologists who were blinded to the clinical and histopathological findings. In case of disagreement, a consensus was reached through discussion. Several quantitative and qualitative parameters were evaluated, including:
Nodule size, shape, and margins
Presence of calcification or cavitation
Iodine concentration within the nodule
Effective atomic number (Z-eff)
Enhancement characteristics in arterial and venous phases
Regions of interest (ROIs) were carefully placed within the nodules, avoiding areas of necrosis, calcification, or adjacent vessels to ensure accurate measurement of iodine uptake.
Reference Standard
The final diagnosis of pulmonary nodules as benign or malignant had been established using histopathological examination, which served as the gold standard. Tissue samples were obtained via CT-guided biopsy, bronchoscopy, or surgical resection, depending on the clinical indication. In cases where biopsy was not feasible, nodules were followed up radiologically for at least six months, and stability or regression was considered indicative of benign pathology.
Data Collection
Demographic data, including age, gender, smoking history, and clinical presentation, had been recorded. Imaging findings from DECT were documented in a structured proforma. Histopathological results and follow-up data were also systematically collected and correlated with imaging findings.
Statistical Analysis
Data had been entered and analyzed using Statistical Package for Social Sciences (SPSS) version 26. Quantitative variables such as iodine concentration and Z-eff values were expressed as mean ± standard deviation, while qualitative variables were presented as frequencies and percentages. Independent sample t-tests were used to compare quantitative variables between benign and malignant nodules.
Receiver Operating Characteristic (ROC) curve analysis had been performed to determine the diagnostic performance of DECT parameters and to identify optimal cutoff values for differentiating benign and malignant lesions. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall diagnostic accuracy were calculated. A p-value of less than 0.05 was considered statistically significant.
Ethical Considerations
The study protocol had been approved by the Institutional Review Board (IRB) of Shifa International Hospital. All procedures had been conducted in accordance with the ethical standards of the institutional research committee and with the principles outlined in the Declaration of Helsinki. Patient confidentiality had been strictly maintained throughout the study.
RESULTS:
Table 1: Baseline Characteristics and Radiological Features of Pulmonary Nodules (n = 110):
| Variable | Benign Nodules (n = 52) | Malignant Nodules (n = 58) | p-value |
| Mean Age (years) | 48.6 ± 12.3 | 61.2 ± 10.5 | <0.001 |
| Gender (Male/Female) | 30 / 22 | 36 / 22 | 0.72 |
| Smoking History (%) | 18 (34.6%) | 39 (67.2%) | <0.001 |
| Nodule Size (mm) | 9.4 ± 3.1 | 16.8 ± 5.2 | <0.001 |
| Location (Upper Lobe %) | 20 (38.5%) | 39 (67.2%) | 0.003 |
| Margin Characteristics | |||
| Smooth | 34 (65.4%) | 9 (15.5%) | <0.001 |
| Lobulated | 10 (19.2%) | 21 (36.2%) | |
| Spiculated | 8 (15.4%) | 28 (48.3%) | |
| Calcification Presence (%) | 28 (53.8%) | 6 (10.3%) | <0.001 |
| Cavitation (%) | 6 (11.5%) | 10 (17.2%) | 0.38 |
| Contrast Enhancement (HU) | 18.5 ± 6.4 | 34.7 ± 9.2 | <0.001 |
Baseline characteristics showed that malignant nodules were significantly associated with older age and a higher prevalence of smoking history. Radiologically, malignant nodules demonstrated larger size, irregular (lobulated or spiculated) margins, and a higher tendency to be located in the upper lobes. In contrast, benign nodules more frequently exhibited smooth margins and calcifications. Contrast enhancement values were significantly higher in malignant lesions, suggesting increased vascularity. These findings highlighted the importance of conventional CT features in initial differentiation, although overlap between groups justified further advanced imaging such as dual-energy CT (DECT).
Table 2: Diagnostic Performance of Dual-Energy CT Parameters in Differentiating Pulmonary Nodules:
| DECT Parameter | Benign Nodules (n = 52) | Malignant Nodules (n = 58) | p-value | Sensitivity (%) | Specificity (%) | Accuracy (%) |
| Iodine Concentration (mg/mL) | 0.9 ± 0.4 | 2.3 ± 0.7 | <0.001 | 89.7 | 84.6 | 87.3 |
| Normalized Iodine Concentration | 0.45 ± 0.15 | 0.88 ± 0.22 | <0.001 | 86.2 | 82.7 | 84.5 |
| Effective Atomic Number (Zeff) | 7.8 ± 0.3 | 8.6 ± 0.5 | <0.001 | 82.8 | 80.8 | 81.8 |
| Slope of Spectral HU Curve | 1.2 ± 0.5 | 3.4 ± 0.9 | <0.001 | 91.4 | 86.5 | 89.1 |
| Virtual Non-Contrast (VNC) HU | 32.5 ± 8.2 | 40.1 ± 9.6 | 0.002 | 75.9 | 73.1 | 74.5 |
| Combined DECT Parameters | — | — | — | 94.8 | 90.4 | 92.7 |
Dual-energy CT parameters demonstrated significant differences between benign and malignant nodules. Malignant nodules exhibited higher iodine concentration, reflecting increased angiogenesis and perfusion. Similarly, normalized iodine concentration and effective atomic number values were elevated in malignant lesions, indicating differences in tissue composition. The slope of the spectral Hounsfield unit curve emerged as one of the most sensitive indicators, reflecting energy-dependent attenuation differences.
Virtual non-contrast values showed modest differentiation but were less reliable compared to contrast-based parameters. Importantly, when multiple DECT parameters were combined, diagnostic performance improved substantially, achieving high sensitivity (94.8%), specificity (90.4%), and overall accuracy (92.7%). This demonstrated that DECT provided a powerful, non-invasive tool for improving diagnostic confidence in distinguishing pulmonary nodules, reducing reliance on invasive biopsy procedures.
DISCUSSION:
The present study evaluated the diagnostic value of dual-energy computed tomography (DECT) in differentiating benign from malignant pulmonary nodules and demonstrated that DECT provided significant incremental value over conventional imaging approaches. The findings suggested that quantitative parameters derived from DECT, particularly iodine concentration and effective atomic number (Z-effective), were instrumental in improving lesion characterization [8]. These parameters reflected tumor vascularity and tissue composition, thereby allowing a more accurate distinction between malignant and benign nodules.
The results of this study were consistent with previous literature, which had highlighted the ability of DECT to assess perfusion-related characteristics of pulmonary lesions. Malignant nodules were observed to exhibit significantly higher iodine uptake compared to benign nodules, likely due to increased neovascularization and angiogenesis [9]. This finding aligned with the biological behavior of malignant tumors, which require enhanced blood supply for rapid growth and metastasis. In contrast, benign lesions, such as granulomas or fibrotic nodules, demonstrated lower iodine concentrations, reflecting limited vascularity.
Furthermore, the study demonstrated that DECT-based material decomposition imaging improved diagnostic confidence. Virtual non-contrast images and iodine maps allowed better visualization of lesion enhancement patterns without the need for additional scanning phases [10]. This not only reduced radiation exposure but also enhanced workflow efficiency. The ability to generate multiple datasets from a single acquisition was particularly advantageous in clinical settings where minimizing patient dose and scan time was essential.
Another important observation was the improved sensitivity and specificity achieved with DECT. The integration of quantitative parameters with morphological assessment reduced the rate of indeterminate nodules, which is a common challenge in routine CT imaging. By providing objective measurements, DECT minimized observer variability and enhanced reproducibility. This was particularly beneficial in borderline cases where conventional CT findings were inconclusive [11].
The study also highlighted the role of DECT in reducing unnecessary invasive procedures. Accurate differentiation between benign and malignant nodules was crucial in guiding clinical decision-making. Patients with benign lesions could be spared from unnecessary biopsies or surgical interventions, while those with malignant nodules could be promptly referred for appropriate oncological management. Thus, DECT contributed to both improved patient outcomes and optimized healthcare resource utilization [12].
Despite these promising findings, certain limitations were acknowledged. The study population was relatively limited, which might have affected the generalizability of the results. Additionally, histopathological confirmation was not available for all cases, and some diagnoses were based on imaging follow-up, which might have introduced a degree of diagnostic uncertainty. Variability in imaging protocols and differences in scanner technology could also influence quantitative measurements, highlighting the need for standardized DECT protocols [13].
Moreover, while DECT showed high diagnostic accuracy, it should not be considered a standalone diagnostic tool. Clinical correlation and integration with other imaging modalities, such as positron emission tomography (PET), remained essential for comprehensive evaluation. Future studies with larger multicenter cohorts and standardized methodologies were recommended to validate these findings and establish definitive cutoff values for DECT parameters [14].
The study demonstrated that DECT had significant diagnostic value in differentiating benign and malignant pulmonary nodules. Its ability to provide both anatomical and functional information enhanced lesion characterization and improved diagnostic accuracy. Although certain limitations existed, DECT was found to be a promising, non-invasive imaging modality that could play an important role in the evaluation and management of pulmonary nodules [15].
CONCLUSION:
The present study concluded that dual-energy computed tomography (DECT) had demonstrated significant diagnostic value in differentiating benign from malignant pulmonary nodules. It had provided enhanced tissue characterization through material decomposition and iodine quantification, allowing for improved assessment of vascularity and lesion composition. The findings indicated that malignant nodules showed higher iodine uptake and distinct spectral attenuation patterns compared to benign lesions, thereby increasing diagnostic confidence. DECT had also reduced the reliance on invasive procedures such as biopsies by offering a non-invasive and reliable alternative for lesion evaluation. Furthermore, it had contributed to earlier and more accurate diagnosis, facilitating timely clinical decision-making and appropriate management strategies. Overall, DECT had proven to be an effective and promising imaging modality in the characterization of pulmonary nodules, with potential to improve patient outcomes and optimize diagnostic pathways in clinical practice.
REFERENCES:
- Friedlander SR, Perez-Johnston R, Wu MY. Challenges in Imaging Pulmonary Nodules: Differentiating Benign from Malignant Lesions. InSeminars in Roentgenology 2025 May 5. WB Saunders.
- Qiu J, Li P, Zhou Y, Zhou X, Zhou Z, Zhou Y, Xu L. Diagnostic value of DLCT multiparametric analysis in differentiating small pulmonary oligometastases from benign lung nodules. Chinese Journal of Academic Radiology. 2026 Mar 12:1-0.
- Ding L, Chen M, Li X, Wu Y, Li J, Deng S, Xu Y, Chen Z, Yan C. Ultra-low dose dual-layer detector spectral CT for pulmonary nodule screening: image quality and diagnostic performance. Insights into Imaging. 2025 Jan 10;16(1):11.
- Yun P, Zhan Z, Wu Z, Rao Y, Sun K, Gong L. The added value of quantitative contrast-enhanced CT parameters in distinguishing malignant from benign solid pulmonary nodules. BMC Medical Imaging. 2025 Jul 24;25(1):294.
- Zhang R, Zheng H, Lin J, Wang J. Review of the application of dual‐energy CT combined with radiomics in the diagnosis and analysis of lung cancer. Journal of Applied Clinical Medical Physics. 2025 Apr;26(4):e70020.
- Zhang J, Lin J, Wang J, Liang Y, Gao C, Zheng H. Application of dual-energy computed tomography combined with radiomics in the clinical diagnosis of lung cancer: a systematic review and meta-analysis. Journal of Thoracic Disease. 2026 Feb 28;18(2):145.
- Yasaka K, Kanzawa J, Inui S, Kubo T, Abe O. Bronchiectasis and airspace enlargement surrounding the lung nodule in dual-energy CT pulmonary angiography: comparison between iodine map and monochromatic image. Radiological Physics and Technology. 2025 Sep;18(3):707-16.
- Durma AD, Saracyn M, Zegadło A, Kamiński G. Successful use of non-contrast dual energy computed tomography in patients with differentiated thyroid cancer. Frontiers in Endocrinology. 2026 Mar 19;17:1742341.
- He J, Du C, Hu M, Zhang J, Cheng Q, Liu Y, Li J, Shen J. Distinguishing benign from malignant thyroid nodules via virtual biopsy: a study on using quantitative parameters and classical radiomics features from dual-energy CT imaging. BMC cancer. 2025 Nov 25;25(1):1823.
- Lin Z, Liu Y, Xia C, Huang P, Peng Z, Yi L, Wang Y, Yu X, Fan B, Zuo M. Dual-energy CT radiomics combined with quantitative parameters for differentiating lung adenocarcinoma from squamous cell carcinoma: A Dual-center study. Academic Radiology. 2025 Mar 1;32(3):1675-84.
- Zhou W, Qu S, Guo ZZ, Qiao WD, Sun TX, Xu SY, Zhao XD, Lu X, Liu XY. The capacity of subtraction CT iodine maps to improve the differentiation of solitary pulmonary nodules. Quantitative Imaging in Medicine and Surgery. 2025 Nov 1;15(11):11336-50.
- Shi J, Shao J, Lin M, Huang Y, Wang L, Chen H, Cao Y, Zhang J, Tan Y, Yu H, Wang X. Diagnostic value of dual-energy CT in differential diagnosis of osteoblastic metastasis and bone islands.
- Fujisaki R, Kawano M, Shirieda K, Matsui T, Komi M, Sato Y, Maeda R, Yanagi S, Kuga N, Uchiyama Y, Azuma M. Differentiation of Solitary Pulmonary Nodules from Benign to Malignant Using Non-contrast Dual Energy CT Electron Density Values. Japanese Journal of Radiological Technology. 2025;81(10):25-1557.
- Tunlayadechanont P, Sananmuang T. Dual-energy CT in head and neck applications. The Neuroradiology Journal. 2025 Oct;38(5):543-52.
- Feng Y, Xu Y, Wang J, Cao Z, Liu B, Du Z, Zhou L, Hua H, Wang W, Mei J, Lai L. Prediction of Early Recurrence After Bronchial Arterial Chemoembolization in Non-small Cell Lung Cancer Patients Using Dual-energy CT: An Interpretable Model Based on SHAP Methodology. Academic Radiology. 2025 Aug 9.
